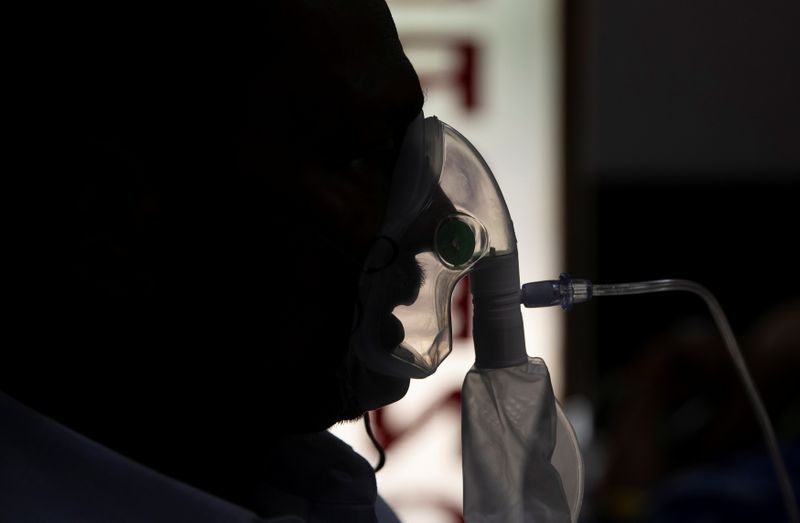
NEW DELHI (Reuters) -India has recorded the world’s sharpest spike in coronavirus infections this month, with political and financial capitals New Delhi and Mumbai running out of hospital beds, oxygen and medicines.
Scientists are studying what led to the unexpected surge, and particularly whether a coronavirus variant first detected in India is to blame. The variant, named B.1.617, has been reported in at least 26 countries, raising global concern. Here are the basics:
WHAT IS THE INDIAN VARIANT?
The B.1.617 variant contains two key mutations to the outer “spike” portion of the virus that attaches to human cells, said senior Indian virologist Shahid Jameel.
The World Health Organization (WHO) said the predominant lineage of B.1.617 was first identified in India last December, although an earlier version was spotted in October 2020.
The U.N. agency and Britain have classified it as a “variant of concern”, along with variants first detected in Britain, Brazil and South Africa. Some initial studies showed the Indian variant spreads more easily.
“There is increased transmissibility demonstrated by some preliminary studies,” Maria Van Kerkhove, WHO’s technical lead on COVID-19, said on May 10, adding that more information is needed about the Indian variant to understand how much of it is circulating.
British health officials said on May 7 there was evidence it spreads more quickly than the original version of the virus and could spread as quickly as the so-called “Kent” variant which fuelled England’s second wave of infections.
ARE VARIANTS DRIVING THE SURGE IN CASES?
It’s hard to say.
Laboratory-based studies of limited sample size suggest potential increased transmissibility, according to the WHO.
The picture is complicated because the highly transmissible B.117 variant first detected in the UK is behind spikes in some parts of India. In New Delhi, UK variant cases almost doubled during the second half of March, according to Sujeet Kumar Singh, director of the National Centre for Disease Control. The Indian variant, though, is widely present in Maharashtra, the country’s hardest-hit state, Singh said.
Prominent U.S. disease modeller Chris Murray, from the University of Washington, said the sheer magnitude of infections in India in a short period of time suggests an “escape variant” may be overpowering any prior immunity from natural infections in those populations.
“That makes it most likely that it’s B.1.617,” he said. But Murray cautioned that gene sequencing data on the coronavirus in India is sparse, and that many cases are also being driven by the UK and South African variants.
Carlo Federico Perno, Head of Microbiology and Immunology Diagnostics at Rome’s Bambino Gesù Hospital, said the Indian variant couldn’t alone be the reason for India’s huge surge, pointing instead to large social gatherings.
Prime Minister Narendra Modi has been criticised for allowing massive political rallies and religious festivals which have been super-spreader events in recent weeks.
DO VACCINES STOP IT?
One bright spot is that vaccines may be protective. White House chief medical adviser Anthony Fauci said that preliminary evidence from lab studies suggest Covaxin, a vaccine developed in India, appears capable of neutralizing the variant.
A double dose of COVID-19 vaccines developed by Pfizer-BioNTech and AstraZeneca is almost as effective against the variant as it is against Britain’s dominant strain, English health officials said on May 22.
Two doses of Pfizer’s shot was 88% effective against symptomatic disease from the variant and AstraZeneca’s was 60% effective, the research showed.
Public Health England is working with international partners but that there is currently no evidence that the Indian variant and two related variants cause more severe disease or render the vaccines currently deployed less effective.
The WHO has said https://bit.ly/3upM84u early studies suggest some loss of vaccines’ neutralisation capacity against the variant, but it is not clear if this translates into decreased vaccine efficacy.
“We don’t have anything to suggest that our diagnostics, our therapeutics and our vaccines don’t work. This is important,” said Van Kerkhove at WHO.
(Reporting by Devjyot Ghoshal and Zeba Siddiqui in New Delhi, Emilio Parodi in Milan, Julie Steenhuysen in Chicago, Stephanie Ulmer-Nebehay in Geneva and Alistair Smout in Britain; Editing by Miyoung Kim, Peter Henderson, Raju Gopalakrishnan, Josephine Mason and Giles Elgood)